
Journal of Emergency Health Care
Formerly known as: International Journal of Medical Investigation

Volume 14, Issue 1 (2-2025)
J Emerg Health Care 2025, 14(1): 0-0 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mahmoudi E, pournajaf A, jalounejad A H, bagheri T, seyedmajidi S, Ghafari M Z. Comparison of Bacterial Microleakage of two Methods of Single Cone Filling and Lateral Compression with two Sealers AH26 and Endoseal MTA. J Emerg Health Care 2025; 14 (1) : 2
URL: http://intjmi.com/article-1-1247-en.html
URL: http://intjmi.com/article-1-1247-en.html
Elham Mahmoudi 

 , Abazar Pournajaf , Amir hosein Jalounejad , Tasnim Bagheri , Seyedali Seyedmajidi , Mahya Zahra Ghafari *
, Abazar Pournajaf , Amir hosein Jalounejad , Tasnim Bagheri , Seyedali Seyedmajidi , Mahya Zahra Ghafari *
, Abazar Pournajaf , Amir hosein Jalounejad , Tasnim Bagheri , Seyedali Seyedmajidi , Mahya Zahra Ghafari *
Endodontics Resident, Department of Endodontics, School of Dentistry, Babol University of Medical Sciences,Mazandaran,Iran
Full-Text [PDF 430 kb]
(423 Downloads)
| Abstract (HTML) (1589 Views)
In another study, Lin et al showed that the lowest amount of microleakage was observed in the teeth filled with EndoSeal MTA and then in the samples filled with BioRoot RCS. They reported that bioceramic sealers of EndoRez sealer with resin base and Sealapex with calcium hydroxide base had better sealing ability(8). In the studies of Drukteinis et al (18) and Adanir et al (19). no significant difference was observed between EndoRez and AH26 or AH Plus;
For this reason, it can be said that based on the results of Lin et al.'s study, EndoSeal MTA and BioRoot RCS bioceramic sealers performed better than resin sealers in terms of sealing ability, which contradicts the results of the present study (8). Due to the fact that the sealers studied in their research are different from the current study, the difference in the results can be investigated. Also, microleakage has been investigated in their study using the glucose penetration test method. The fact that glucose molecules are smaller than the size of Enterococcus faecalis bacteria can play a role in the difference between the reported results.
In another article, Bahlke et al showed that the apical microleakage of Endoseal MTA was significantly less than AH Plus. Despite the fact that AH Plus was used in Bahleke's study, unlike the present study, both AH26 and AH Plus sealers have a resin base, and according to the studies of Durkteinis et al. and Adanir et al., no significant difference was observed between the performance of these two sealers (6, 18, 19). Based on this, it can be said that the results of Bahlke's study are in conflict with the present study.
This conflict can be related to the microleakage investigation method, in their study unlike the present study, dye penetration test was used. Color molecules are smaller than Enterococcus faecalis bacteria. Also, considering the possibility of color penetration through the dentin tubules, the difference in the amount of microleakage in the Bahleh study and the present study may be justified. In addition, the method of investigating microleakage in the present study into the oral environment (infiltration of bacteria from coronal to apical) is more similar to the oral environment than the study by Bahlke et al. (infiltration of dye from the tooth apex).
Based on the results of the present study, in the use of any type of sealer, the single cone method had less microleakage than the lateral compaction method. However, no significant difference was observed between them. In the study conducted by Sami et al., they did not observe any significant difference between these two methods(20). In another study, Mobarak et al showed that the single cone method using bioceramic sealer produced a better seal than the lateral compression method with resin sealers. Of course, in this study, unlike the current study, a significant difference was observed between the single cone method and lateral density (4). The reason for this can be related to the different type of sealers used in the study by Mobarak et al compared to the present study; They used Endosequence bioceramic sealer in single cone method and Adseal resin sealer and Endosequence bioceramic sealer and MTA Fillapex in lateral compression method. This study also reported another result that the lateral density filling method with bioceramic sealer (MTA Fillapex) had the lowest sealing ability. Therefore, it is likely that bioceramic sealers with the single cone filling method have better results than the lateral compression method, which is in line with our study(4).
According to the manufacturer's instructions, bioceramic sealers are designed to be used with the single cone method, and the spreader does not have good penetration power in them; As a result, the number of sub-cans is reduced. Also, the influence of the spreader reduces the volume of the sealer around the gutta, which may justify the preference of the single cone method over lateral compaction. To check the validity of this hypothesis, more studies are needed to compare the effect of the root filling method on sealing ability with different bioceramic sealers.
Despite the fact that the average duration of microleakage in the AH26 group using the single cone method was higher than other groups, no significant relationship was found between the average duration of microleakage between the groups of this study. Similar to our study, Milani et al The article itself stated that there was no significant difference between the studied groups in terms of the rate of occurrence of microleakage during the study period; However, at the end of their study, a statistically significant difference was seen between the occurrence of microleakage in different groups (17). Also, in the study of Yanpiset et al., no significant difference was observed in terms of the average duration of microleakage in different groups.
They concluded that within 60 days, there was no significant difference between the studied groups in terms of the speed and amount of bacterial microleakage, and the performance of these methods was equal, which is the same as the present study(2).
Conclusion
Considering the limitations of this study, no difference was observed in the use of AH26 and Endoseal MTA sealers with single cone and lateral compression methods in preventing bacterial microleakage. However, it seems that for Endoseal MTA sealer, using the single cone method will bring better results.
Conflict of interest
There is no conflict of interest related to the authors of the article.
Ethics statement
The article has the code of ethics IR.MUBABOL.REC.1400.177 and Written informed consent was obtained from the individuals for the publication of any potentially identifiable data included in this article.
Full-Text: (464 Views)
Introduction
Proper endodontics treatment with knowledge of the morphology of the root canal includes cleaning and shaping and finally correct filling using a suitable sealer (1).The main purpose of filling the root canal is to create a complete flood to prevent contamination and re-infection due to leakage of liquids and microorganisms into the root canal (2).The most common root canal filling material is gutta-percha, which is used in different ways, including lateral compression, vertical compression, and thermoplastic(3).
The use of sealer is very important for long-term sealing of the root canal, because it adheres to the gutta-percha and the dentin of the root canal and fills the irregularities and spaces between the gutta-percha and the walls of the root canal (4). Root canal sealers are effective in completely filling the root canal by reducing apical and coronal microleakage (5). In all root canal filling methods, the dentist must use a type of sealer to improve the filling quality, which depends on the sealing ability of the used sealer(6).
Currently, there are various types of sealers, including zinc oxide, eugenol, calcium hydroxide, glass ionomer, silicone, resin, and bioceramic sealers (7).Recently, bioceramic materials have become one of the most famous biological materials used in endodontics after the clinical success of MTA. Bioceramic sealers have various advantages such as low cytotoxicity, excellent antimicrobial activity due to high pH, stimulation of hard tissue formation and formation of hydroxyapatite layer (8).Endoseal MTA is a type of bioceramic sealer that has been introduced recently and contains a pre-mixed material that is kept in a syringe under vacuum conditions and allows its direct use inside the root canals (7). This sealer consists of calcium silicate, calcium aluminate, calcium aluminoferrite and calcium sulfate(9). During setting, the moisture is absorbed by the sealer and it sets slowly without any mixing(10).
Among some desirable mechanical and biological properties of Endoseal MTA, we can mention biocompatibility, greater resistance to washing, and bioactivity(11). On the other hand, this sealer has disadvantages such as color change due to the release of iron ions, long stinging, short working time and hard work. Also, there is no known solvent for MTA; Therefore, it is difficult to remove it from the root canal (7).
On the other hand, epoxy resin-based sealers are used in the root of the tooth as a standard gold, and with changes to the original formula, they are widely used to fill the root canal (3). Resin sealers have a greater penetration depth than ordinary sealers (12). Due to their low layer thickness, these sealers have deeper penetration and good fluidity. Also, resin sealers have high bond strength to dentin (13).
As one of the resin sealers, AH26 has good sealing power and adhesive properties and antibacterial properties (14). It has been confirmed that AH26 releases formaldehyde when it sets. These sealers do not contain formaldehyde in their chemical composition, but during the chemical reactions that occur when they are set, formaldehyde is produced and released, which is an effective substance against bacteria (15). It has been reported that AH26 sealer can maintain its antibacterial property from 24 hours to 7 days (16).
Due to the fact that Endoseal MTA is one of the newer sealers and sufficient studies were not found in the field of comparing the performance of this sealer with standard gold sealers, this study considered the bacterial microleakage of two sealers, AH26 and Endoseal MTA, with two methods of single cone filling and lateral compression.
Methods
In order to carry out this laboratory study (in vitro), according to the formula for determining the sample size, taking into account the α error of 0.05 and the β error of 0.20 and the results of previous similar studies, the minimum number of samples in each group was determined to be 14.56 extracted single-rooted human teeth, which were matched in terms of tooth type, were collected from clinics and dental offices in Mazandaran.Single-root and single-canal teeth with developed apex, without external analysis, without cracks on the root surface, without caries and without additional canal were included in the study. This project was implemented with the code of ethics IR.MUBABOL.REC.1400.177.In order to remove mass and soft tissue on the root surface, all teeth were mechanically cleaned with periodontal cort and placed in 5.25% sodium hypochlorite solution for one hour and placed in distilled water until use.
In order to homogenize the samples, the crown of the teeth was cut using a turbine and a diamond bur, so that 12 mm of each tooth remained. In order to remove the variable related to the operator, all preparation steps were done by one person.
Preparation of teeth
k-file (Mani inc, Tochigi, Japan) number 15 was used to determine the working length. In this way, the file was placed in the canal until the tip of the file was seen in the apical foramen. Then the working length was determined to be 1 mm less than this length. To prepare the root canal of the teeth, Sx to F3 nickel titanium (Ni-Ti) rotary files from the Protaper gold system (Dentsply Maillefer, Ballaigues, Switzerland) were used. To maintain patency in the filing intervals between each step and the next step, the canal was washed using 1 ml of 25.5% sodium hypochlorite and 5 ml of sterile physiological serum 0.9%, and then a manual file No. 10 was inserted along the length of the canal to remove debris. come out from the end of the apex of the root.
After preparing the canals, the teeth were sterilized by UV rays (4) and after the sterilization process in all four experimental groups of root canals, they were dried using a paper cone (Ariadent, Iran). Then the teeth were randomly divided into four groups:
1. Group one: 14 teeth filled with gutta-percha and AH26 sealer by single-cone method.
2. Group two: 14 teeth filled with gutta percha and AH26 sealer by lateral compression method.
3. Group three: 14 teeth that were filled with gutta percha and Endoseal MTA sealer by single-cone method.
4. Group four: 14 teeth that were filled with gutta percha and Endoseal MTA sealer by lateral compression method.
In each group, one tooth was placed as a positive control and one tooth as a negative control. Positive and negative control were considered as follows:
- Negative control: teeth that were prepared and filled with AH26 sealer by lateral compression method, but were not exposed to bacteria.
- Positive control: a tooth that was prepared but not filled.
AH26 sealer was stirred on a glass slab until a homogeneous consistency was obtained and it was applied to the canal wall using Maillefer (Dentsply, Switzerland) spreader No. In the single-cone method, an F3 (Meta biomed, Korea) along with the pumping movement was placed inside the canal, in such a way that the excess sealer was removed from the canal opening.
Then the additions of the sealer were removed and the gutta was cut and compacted. Also, in the lateral compression method, the original gutta-percha with a tipper of 2% (Meta biomed, Korea) was selected as MAC according to the last apical file used, that is, gutta-percha No. 30 or larger than the one that had a tug back function during a brief operation. The largest finger spreader that reached 1 mm length in the presence of MAC
was selected and secondary gutta-percha (Ariadent, Iran) was used for filling by lateral compression method. Gutta-percha sub-cones were used until the spreader penetrated more than 2 mm beyond the canal entrance. After the filling was completed, a heat carrier was used to cut the gutta-percha and remove the excess gutta-percha. Then the gutta-percha was compacted with Dentsply, Maillefer plugger (Switzerland). After completing the filling, radiographs were prepared from the samples to evaluate the filling quality. Then, all the teeth in the experimental groups were kept in 100% humidity and 37°C temperature for 1 week until the sealer set.
Preparation of samples to check microleakage
The outer surface of all the teeth of the experimental groups except for 1 mm of the apical end was covered with two layers of nail polish (Arcancil, France). In the negative control teeth, the entire external surface of the root, including the apical foramen and the canal entrance, was covered with two layers of nail polish. In the positive control teeth, the entire surface of the tooth was varnished except for the apical and coronal 1 mm. The separate chamber model was used to investigate bacterial leakage using bacterial suspension; Thus, the upper chamber containing the coronal third of the root was in contact with the bacterial suspension and the lower chamber containing the apical two thirds of the root was placed in contact with the TSB culture medium. Micropipettes with a volume of 0.5 cc with an inner diameter of 7 mm and a length of 30 mm were used to create the upper chamber in the coronal part of each tooth.
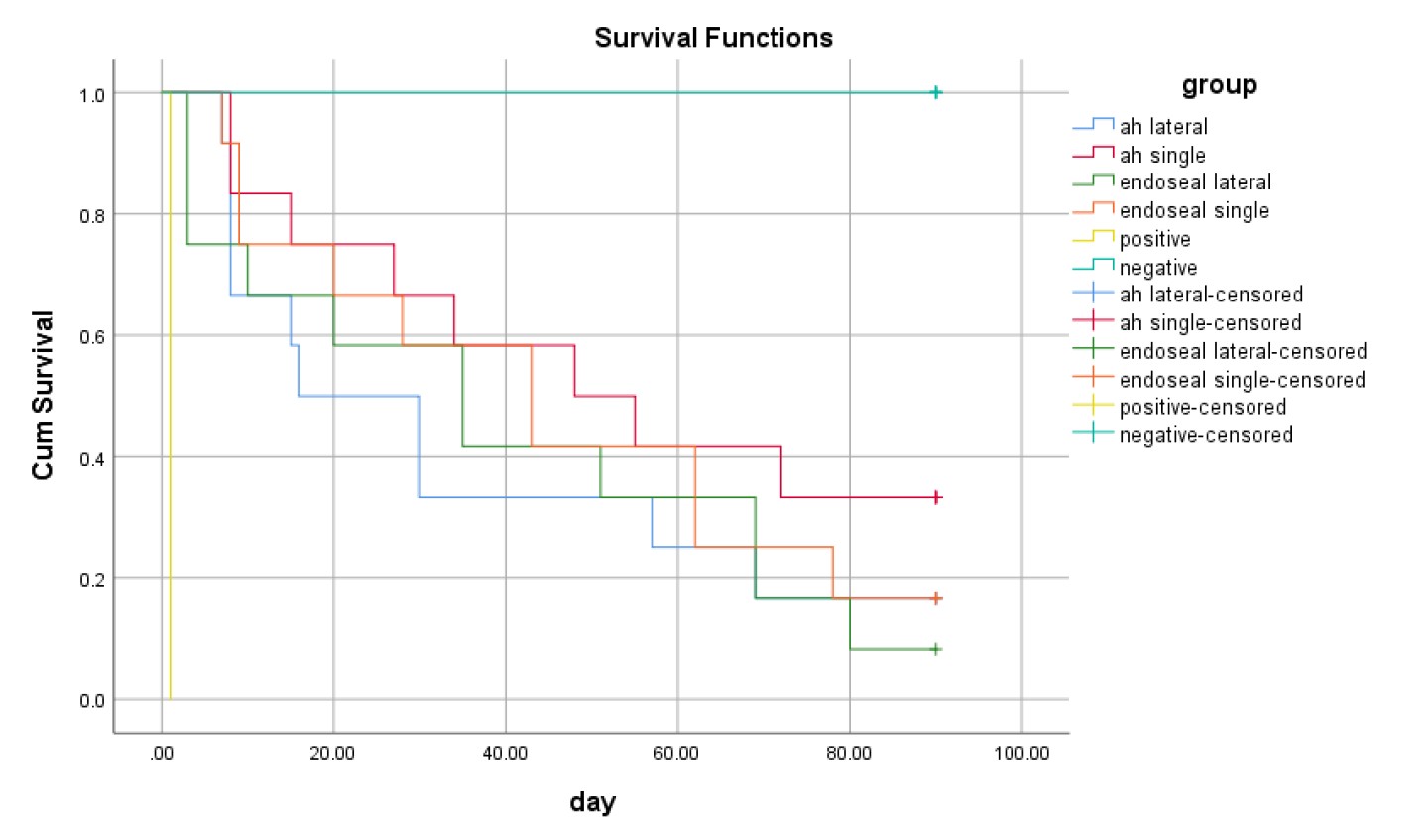
The ends of the micropipettes were cut and the coronal third of the root was placed inside the cut end of the micropipette. The junction between the micropipette and the root was sealed with cyanoacrylate glue. A test vial was used to create the lower chamber in the apical part of the root. The dimensions of these vials were 50 mm (height) x 10 mm (diameter) and had a volume capacity of 2 cc and had a plastic lid. First, the lid of these vials was removed, and using an electric drill and a drill, a hole with a diameter of 7 mm (the size of a micropipette) was created in the middle of the vial lid. Then the micropipette was passed through the created hole and the joint of the micropipette and the cap of the test vial was completely sealed with glue. Finally, the cap containing the micropipette and the tooth root were placed on the vial. The samples were sterilized by UV rays (4).(Figure 1).
After sterilization, the samples were removed from the cover and after opening the cap of the vial, sterile liquid culture medium Tryptic Soy Broth (TSB) (Merk, Germany) was poured into the lower chamber using a sterile 22-gauge syringe and needle. Be in contact with the apical 2 mm of the root that was not covered with nail polish. To prepare liquid TSB culture medium, according to the instructions of the manufacturer, 30 grams of its powder was dissolved in 1000 cc of distilled water, then poured into a sterile Erlen (Razi, Iran) and autoclaved (temperature 121 15 minutes) was sterilized.
After performing this step, all the samples were kept in an incubator at 37°C for 72 hours to ensure the sterility of the set; In this way, the absence of turbidity in the culture medium indicated the absence of contamination of the samples.
Bacterial leakage
Enterococcus faecalis (ATCC29212) was used to obtain the bacterial suspension. A suspension containing 109 bacteria was prepared from Enterococcus faecalis in TSB culture medium and 0.3 ml of the above suspension was injected into the upper chamber using a sterile syringe and needle. Then, these collections were incubated at 37°C for a maximum of 90 days and checked every day for the presence of turbidity in the TSB culture medium (lower compartment). The turbidity of the culture medium indicated microbial leakage along the root canal into the underlying culture medium. In each sample, the time it took (in days) for turbidity to appear in the bottom culture medium was recorded. In addition, the bacterial solution was changed every 3 days to ensure the presence of live and active microorganisms. After observing the turbidity of the culture medium, one sample was randomly selected from among the samples with cloudy culture medium in each group. Then, observing the sterile conditions and in the vicinity of the flame under the hood, the vials were opened and samples were taken by a sterile analyzer (Razi, Iran).
 Figure 1. How to design compartments
Figure 1. How to design compartments
The removed sample was cultured in blood agar solid culture medium (Difco, Germany) to check the presence of microorganisms and possible contamination. The blood agar medium was incubated at 37°C for 48 hours. Then the grown colonies were sampled and warm staining was done. The stained samples were examined under the microscope with 100x magnification (Figure 2).
Finally, the data was entered into SPSS software version 22 and Kruskal-Wallis, chi-square and Kaplan-Meier statistical analysis by log-rank test (mantel-cox) were used to analyze the data. P-value < 0.05 was considered statistically significant.
Proper endodontics treatment with knowledge of the morphology of the root canal includes cleaning and shaping and finally correct filling using a suitable sealer (1).The main purpose of filling the root canal is to create a complete flood to prevent contamination and re-infection due to leakage of liquids and microorganisms into the root canal (2).The most common root canal filling material is gutta-percha, which is used in different ways, including lateral compression, vertical compression, and thermoplastic(3).
The use of sealer is very important for long-term sealing of the root canal, because it adheres to the gutta-percha and the dentin of the root canal and fills the irregularities and spaces between the gutta-percha and the walls of the root canal (4). Root canal sealers are effective in completely filling the root canal by reducing apical and coronal microleakage (5). In all root canal filling methods, the dentist must use a type of sealer to improve the filling quality, which depends on the sealing ability of the used sealer(6).
Currently, there are various types of sealers, including zinc oxide, eugenol, calcium hydroxide, glass ionomer, silicone, resin, and bioceramic sealers (7).Recently, bioceramic materials have become one of the most famous biological materials used in endodontics after the clinical success of MTA. Bioceramic sealers have various advantages such as low cytotoxicity, excellent antimicrobial activity due to high pH, stimulation of hard tissue formation and formation of hydroxyapatite layer (8).Endoseal MTA is a type of bioceramic sealer that has been introduced recently and contains a pre-mixed material that is kept in a syringe under vacuum conditions and allows its direct use inside the root canals (7). This sealer consists of calcium silicate, calcium aluminate, calcium aluminoferrite and calcium sulfate(9). During setting, the moisture is absorbed by the sealer and it sets slowly without any mixing(10).
Among some desirable mechanical and biological properties of Endoseal MTA, we can mention biocompatibility, greater resistance to washing, and bioactivity(11). On the other hand, this sealer has disadvantages such as color change due to the release of iron ions, long stinging, short working time and hard work. Also, there is no known solvent for MTA; Therefore, it is difficult to remove it from the root canal (7).
On the other hand, epoxy resin-based sealers are used in the root of the tooth as a standard gold, and with changes to the original formula, they are widely used to fill the root canal (3). Resin sealers have a greater penetration depth than ordinary sealers (12). Due to their low layer thickness, these sealers have deeper penetration and good fluidity. Also, resin sealers have high bond strength to dentin (13).
As one of the resin sealers, AH26 has good sealing power and adhesive properties and antibacterial properties (14). It has been confirmed that AH26 releases formaldehyde when it sets. These sealers do not contain formaldehyde in their chemical composition, but during the chemical reactions that occur when they are set, formaldehyde is produced and released, which is an effective substance against bacteria (15). It has been reported that AH26 sealer can maintain its antibacterial property from 24 hours to 7 days (16).
Due to the fact that Endoseal MTA is one of the newer sealers and sufficient studies were not found in the field of comparing the performance of this sealer with standard gold sealers, this study considered the bacterial microleakage of two sealers, AH26 and Endoseal MTA, with two methods of single cone filling and lateral compression.
Methods
In order to carry out this laboratory study (in vitro), according to the formula for determining the sample size, taking into account the α error of 0.05 and the β error of 0.20 and the results of previous similar studies, the minimum number of samples in each group was determined to be 14.56 extracted single-rooted human teeth, which were matched in terms of tooth type, were collected from clinics and dental offices in Mazandaran.Single-root and single-canal teeth with developed apex, without external analysis, without cracks on the root surface, without caries and without additional canal were included in the study. This project was implemented with the code of ethics IR.MUBABOL.REC.1400.177.In order to remove mass and soft tissue on the root surface, all teeth were mechanically cleaned with periodontal cort and placed in 5.25% sodium hypochlorite solution for one hour and placed in distilled water until use.
In order to homogenize the samples, the crown of the teeth was cut using a turbine and a diamond bur, so that 12 mm of each tooth remained. In order to remove the variable related to the operator, all preparation steps were done by one person.
Preparation of teeth
k-file (Mani inc, Tochigi, Japan) number 15 was used to determine the working length. In this way, the file was placed in the canal until the tip of the file was seen in the apical foramen. Then the working length was determined to be 1 mm less than this length. To prepare the root canal of the teeth, Sx to F3 nickel titanium (Ni-Ti) rotary files from the Protaper gold system (Dentsply Maillefer, Ballaigues, Switzerland) were used. To maintain patency in the filing intervals between each step and the next step, the canal was washed using 1 ml of 25.5% sodium hypochlorite and 5 ml of sterile physiological serum 0.9%, and then a manual file No. 10 was inserted along the length of the canal to remove debris. come out from the end of the apex of the root.
After preparing the canals, the teeth were sterilized by UV rays (4) and after the sterilization process in all four experimental groups of root canals, they were dried using a paper cone (Ariadent, Iran). Then the teeth were randomly divided into four groups:
1. Group one: 14 teeth filled with gutta-percha and AH26 sealer by single-cone method.
2. Group two: 14 teeth filled with gutta percha and AH26 sealer by lateral compression method.
3. Group three: 14 teeth that were filled with gutta percha and Endoseal MTA sealer by single-cone method.
4. Group four: 14 teeth that were filled with gutta percha and Endoseal MTA sealer by lateral compression method.
In each group, one tooth was placed as a positive control and one tooth as a negative control. Positive and negative control were considered as follows:
- Negative control: teeth that were prepared and filled with AH26 sealer by lateral compression method, but were not exposed to bacteria.
- Positive control: a tooth that was prepared but not filled.
AH26 sealer was stirred on a glass slab until a homogeneous consistency was obtained and it was applied to the canal wall using Maillefer (Dentsply, Switzerland) spreader No. In the single-cone method, an F3 (Meta biomed, Korea) along with the pumping movement was placed inside the canal, in such a way that the excess sealer was removed from the canal opening.
Then the additions of the sealer were removed and the gutta was cut and compacted. Also, in the lateral compression method, the original gutta-percha with a tipper of 2% (Meta biomed, Korea) was selected as MAC according to the last apical file used, that is, gutta-percha No. 30 or larger than the one that had a tug back function during a brief operation. The largest finger spreader that reached 1 mm length in the presence of MAC
was selected and secondary gutta-percha (Ariadent, Iran) was used for filling by lateral compression method. Gutta-percha sub-cones were used until the spreader penetrated more than 2 mm beyond the canal entrance. After the filling was completed, a heat carrier was used to cut the gutta-percha and remove the excess gutta-percha. Then the gutta-percha was compacted with Dentsply, Maillefer plugger (Switzerland). After completing the filling, radiographs were prepared from the samples to evaluate the filling quality. Then, all the teeth in the experimental groups were kept in 100% humidity and 37°C temperature for 1 week until the sealer set.
Preparation of samples to check microleakage
The outer surface of all the teeth of the experimental groups except for 1 mm of the apical end was covered with two layers of nail polish (Arcancil, France). In the negative control teeth, the entire external surface of the root, including the apical foramen and the canal entrance, was covered with two layers of nail polish. In the positive control teeth, the entire surface of the tooth was varnished except for the apical and coronal 1 mm. The separate chamber model was used to investigate bacterial leakage using bacterial suspension; Thus, the upper chamber containing the coronal third of the root was in contact with the bacterial suspension and the lower chamber containing the apical two thirds of the root was placed in contact with the TSB culture medium. Micropipettes with a volume of 0.5 cc with an inner diameter of 7 mm and a length of 30 mm were used to create the upper chamber in the coronal part of each tooth.
The ends of the micropipettes were cut and the coronal third of the root was placed inside the cut end of the micropipette. The junction between the micropipette and the root was sealed with cyanoacrylate glue. A test vial was used to create the lower chamber in the apical part of the root. The dimensions of these vials were 50 mm (height) x 10 mm (diameter) and had a volume capacity of 2 cc and had a plastic lid. First, the lid of these vials was removed, and using an electric drill and a drill, a hole with a diameter of 7 mm (the size of a micropipette) was created in the middle of the vial lid. Then the micropipette was passed through the created hole and the joint of the micropipette and the cap of the test vial was completely sealed with glue. Finally, the cap containing the micropipette and the tooth root were placed on the vial. The samples were sterilized by UV rays (4).(Figure 1).
After sterilization, the samples were removed from the cover and after opening the cap of the vial, sterile liquid culture medium Tryptic Soy Broth (TSB) (Merk, Germany) was poured into the lower chamber using a sterile 22-gauge syringe and needle. Be in contact with the apical 2 mm of the root that was not covered with nail polish. To prepare liquid TSB culture medium, according to the instructions of the manufacturer, 30 grams of its powder was dissolved in 1000 cc of distilled water, then poured into a sterile Erlen (Razi, Iran) and autoclaved (temperature 121 15 minutes) was sterilized.
After performing this step, all the samples were kept in an incubator at 37°C for 72 hours to ensure the sterility of the set; In this way, the absence of turbidity in the culture medium indicated the absence of contamination of the samples.
Bacterial leakage
Enterococcus faecalis (ATCC29212) was used to obtain the bacterial suspension. A suspension containing 109 bacteria was prepared from Enterococcus faecalis in TSB culture medium and 0.3 ml of the above suspension was injected into the upper chamber using a sterile syringe and needle. Then, these collections were incubated at 37°C for a maximum of 90 days and checked every day for the presence of turbidity in the TSB culture medium (lower compartment). The turbidity of the culture medium indicated microbial leakage along the root canal into the underlying culture medium. In each sample, the time it took (in days) for turbidity to appear in the bottom culture medium was recorded. In addition, the bacterial solution was changed every 3 days to ensure the presence of live and active microorganisms. After observing the turbidity of the culture medium, one sample was randomly selected from among the samples with cloudy culture medium in each group. Then, observing the sterile conditions and in the vicinity of the flame under the hood, the vials were opened and samples were taken by a sterile analyzer (Razi, Iran).
Figure 1. How to design compartmentsThe removed sample was cultured in blood agar solid culture medium (Difco, Germany) to check the presence of microorganisms and possible contamination. The blood agar medium was incubated at 37°C for 48 hours. Then the grown colonies were sampled and warm staining was done. The stained samples were examined under the microscope with 100x magnification (Figure 2).
Figure 2. Examining stained bacteria under a microscope with 100x magnification
Finally, the data was entered into SPSS software version 22 and Kruskal-Wallis, chi-square and Kaplan-Meier statistical analysis by log-rank test (mantel-cox) were used to analyze the data. P-value < 0.05 was considered statistically significant.
Table 1. The number and percentage of occurrence of microleakage in each group
* chi-square
Table 2. Mean and standard error of microleakage in each group
* Kruskal-Wallis test
| microleakage Group |
Abundance |
percentage |
P-value* | |
| AH26 | Lateral compression |
10 | 83.3% | 0.468 |
| Single cone |
8 | 66.7% | ||
| Endoseal MTA | Lateral compression |
11 | 91.7% | |
| Single cone |
10 | 83.3% | ||
Table 2. Mean and standard error of microleakage in each group
| Microleakage Group |
Average Day |
Standard Error |
95% Confidence Interval of the Mean |
P-value* | ||
| lower limit |
upper limit |
|||||
| AH26 | Lateral compression |
35.67 | 8.92 | 18/18 | 53/16 | 0.467 |
| Single cone |
52.25 | 9.28 | 34/07 | 70/43 | ||
| Endoseal MTA | Lateral compression |
39 | 8.88 | 21/6 | 56/4 | |
| Single cone |
45.08 | 8.61 | 28/21 | 61/96 | ||
Results
The highest number of teeth that suffered microleakage in the 90-day interval was observed in the Endoseal MTA group using the lateral compression method (91.7%) and the lowest number of microleakage was observed in the AH26 group using the single cone method (66.7%); However, no statistically significant relationship was found in terms of the number of microleakage occurrences and the studied groups (P=0.468) (Table 1). In this study, positive control samples of all four groups showed bacterial microleakage on the first day, but microleakage was not seen in any of the negative control samples.
According to Table 2, the highest average duration of microleakage in the AH26 group was by the single cone method (52.25) and the lowest was in the AH26 group by the lateral compression method (35.66), and the difference was not statistically significant (P= 0.467).
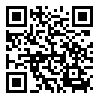
Figure 3 shows the survival rate of samples in each group (the duration of time without the occurrence of microleakage). According to the log-rank test performed by the Kaplan-Meier method, the average survival time difference between the studied groups was not significant (P=0.584).
Discussion
In this study, the lowest frequency of bacterial microleakage was observed in the use of AH26 by the single cone method and the highest frequency was observed in the use of Endoseal MTA by the lateral compression method. Milani et al also reported that MTA Fillapex had the highest frequency of microleakage, which is somewhat consistent with the present study (17).
The highest number of teeth that suffered microleakage in the 90-day interval was observed in the Endoseal MTA group using the lateral compression method (91.7%) and the lowest number of microleakage was observed in the AH26 group using the single cone method (66.7%); However, no statistically significant relationship was found in terms of the number of microleakage occurrences and the studied groups (P=0.468) (Table 1). In this study, positive control samples of all four groups showed bacterial microleakage on the first day, but microleakage was not seen in any of the negative control samples.
According to Table 2, the highest average duration of microleakage in the AH26 group was by the single cone method (52.25) and the lowest was in the AH26 group by the lateral compression method (35.66), and the difference was not statistically significant (P= 0.467).
Figure 3 shows the survival rate of samples in each group (the duration of time without the occurrence of microleakage). According to the log-rank test performed by the Kaplan-Meier method, the average survival time difference between the studied groups was not significant (P=0.584).
Discussion
In this study, the lowest frequency of bacterial microleakage was observed in the use of AH26 by the single cone method and the highest frequency was observed in the use of Endoseal MTA by the lateral compression method. Milani et al also reported that MTA Fillapex had the highest frequency of microleakage, which is somewhat consistent with the present study (17).
Figure 3. Comparison of the average survival time in the studied groups
For this reason, it can be said that based on the results of Lin et al.'s study, EndoSeal MTA and BioRoot RCS bioceramic sealers performed better than resin sealers in terms of sealing ability, which contradicts the results of the present study (8). Due to the fact that the sealers studied in their research are different from the current study, the difference in the results can be investigated. Also, microleakage has been investigated in their study using the glucose penetration test method. The fact that glucose molecules are smaller than the size of Enterococcus faecalis bacteria can play a role in the difference between the reported results.
In another article, Bahlke et al showed that the apical microleakage of Endoseal MTA was significantly less than AH Plus. Despite the fact that AH Plus was used in Bahleke's study, unlike the present study, both AH26 and AH Plus sealers have a resin base, and according to the studies of Durkteinis et al. and Adanir et al., no significant difference was observed between the performance of these two sealers (6, 18, 19). Based on this, it can be said that the results of Bahlke's study are in conflict with the present study.
This conflict can be related to the microleakage investigation method, in their study unlike the present study, dye penetration test was used. Color molecules are smaller than Enterococcus faecalis bacteria. Also, considering the possibility of color penetration through the dentin tubules, the difference in the amount of microleakage in the Bahleh study and the present study may be justified. In addition, the method of investigating microleakage in the present study into the oral environment (infiltration of bacteria from coronal to apical) is more similar to the oral environment than the study by Bahlke et al. (infiltration of dye from the tooth apex).
Based on the results of the present study, in the use of any type of sealer, the single cone method had less microleakage than the lateral compaction method. However, no significant difference was observed between them. In the study conducted by Sami et al., they did not observe any significant difference between these two methods(20). In another study, Mobarak et al showed that the single cone method using bioceramic sealer produced a better seal than the lateral compression method with resin sealers. Of course, in this study, unlike the current study, a significant difference was observed between the single cone method and lateral density (4). The reason for this can be related to the different type of sealers used in the study by Mobarak et al compared to the present study; They used Endosequence bioceramic sealer in single cone method and Adseal resin sealer and Endosequence bioceramic sealer and MTA Fillapex in lateral compression method. This study also reported another result that the lateral density filling method with bioceramic sealer (MTA Fillapex) had the lowest sealing ability. Therefore, it is likely that bioceramic sealers with the single cone filling method have better results than the lateral compression method, which is in line with our study(4).
According to the manufacturer's instructions, bioceramic sealers are designed to be used with the single cone method, and the spreader does not have good penetration power in them; As a result, the number of sub-cans is reduced. Also, the influence of the spreader reduces the volume of the sealer around the gutta, which may justify the preference of the single cone method over lateral compaction. To check the validity of this hypothesis, more studies are needed to compare the effect of the root filling method on sealing ability with different bioceramic sealers.
Despite the fact that the average duration of microleakage in the AH26 group using the single cone method was higher than other groups, no significant relationship was found between the average duration of microleakage between the groups of this study. Similar to our study, Milani et al The article itself stated that there was no significant difference between the studied groups in terms of the rate of occurrence of microleakage during the study period; However, at the end of their study, a statistically significant difference was seen between the occurrence of microleakage in different groups (17). Also, in the study of Yanpiset et al., no significant difference was observed in terms of the average duration of microleakage in different groups.
They concluded that within 60 days, there was no significant difference between the studied groups in terms of the speed and amount of bacterial microleakage, and the performance of these methods was equal, which is the same as the present study(2).
In the present study, positive and negative control samples were used in each group to check the correct design of the sample model for testing. The negative control sample using cyanoacrylate varnish and glue showed that the method of sealing the gaps between different compartments was effective and there was no possibility of bacterial penetration. On the other hand, the positive control sample showed that the penetration of bacteria from the upper compartment through the root canal to the culture medium of the lower compartment was possible.
The results of the present study showed that there is no significant difference between the use of Endoseal MTA and AH26 with the two methods of single cone and lateral compression; Therefore, it can be concluded that within the scope of the results of this study, the use of both AH26 sealer and Endoseal MTA in both side compression and single cone methods is acceptable. However, the results obtained in laboratory studies may not be suitable for direct generalization to clinical situations due to the lack of simulation of PDL and the absence of other clinical parameters (8). However, this study provided results that can be used as a basis for future studies with different sealers. Therefore, in-vivo studies and clinical trials are needed to provide more reliable and valid results.Conclusion
Considering the limitations of this study, no difference was observed in the use of AH26 and Endoseal MTA sealers with single cone and lateral compression methods in preventing bacterial microleakage. However, it seems that for Endoseal MTA sealer, using the single cone method will bring better results.
Conflict of interest
There is no conflict of interest related to the authors of the article.
Ethics statement
The article has the code of ethics IR.MUBABOL.REC.1400.177 and Written informed consent was obtained from the individuals for the publication of any potentially identifiable data included in this article.
References
1. Safai P, Farzaneh B, Fekrazad R. The effects of pressure in vitro on three methods of root canal obturation. Diving and hyperbaric medicine. 2019;49(1):16. https://doi.org/10.28920/dhm49.1.16-20 , PMid:30856663 PMCid:PMC6526054
2. Yanpiset K, Banomyong D, Chotvorrarak K, Srisatjaluk RL. Bacterial leakage and micro-computed tomography evaluation in round-shaped canals obturated with bioceramic cone and sealer using matched single cone technique. Restorative dentistry & endodontics. 2018;43(3).
https://doi.org/10.5395/rde.2018.43.e30, PMid:30135849 PMCid:PMC6103543
3. Kim SR, Kwak SW, Lee JK, Goo HJ, Ha JH, Kim HC. Efficacy and retrievability of root canal filling using calcium silicate‐based and epoxy resin‐based root canal sealers with matched obturation techniques. Australian Endodontic Journal. 2019;45(3):337-45.
https://doi.org/10.1111/aej.12323, PMid:30614168
4. Mobarak A, Moussa S, Zaazou A, Abdelfattah H. Comparison of bacterial coronal leakage between different obturation materials (an in vitro study). Alexandria Dental Journal. 2015;40(1):1-7. https://doi.org/10.21608/adjalexu.2015.56488
5. El Sayed MAAM, Al Husseini H. Apical dye leakage of two single-cone root canal core materials (hydrophilic core material and gutta-percha) sealed by different types of endodontic sealers: An: in vitro: study. Journal of Conservative Dentistry and Endodontics. 2018;21(2):147-52.
https://doi.org/10.4103/JCD.JCD_154_17, PMid:29674815 PMCid:PMC5890403
6. Bahlakeh M, Omidi S, Lomee M, Cherati J. Microleakage assessment of a new mineral trioxide aggregate-based root canal sealer in the presence and absence of saliva. Annals of Dental Specialty. 2018;2018:6.
7. Moazami F, Naseri M, Malekzadeh P. Different application methods for endoseal MTA sealer: a comparative study. Iranian Endodontic Journal. 2020;15(1):44.
8. Lin GSS, Ghani NRNA, Noorani TY, Kamarudin A. Apical sealing ability of different endodontic sealers using glucose penetration test: a standardized methodological approach. Cumhuriyet Dental Journal. 2020;23(2):79-87. https://doi.org/10.7126/cumudj.704107
9. Kim S, Kim S, Park J-W, Jung I-Y, Shin S-J. Comparison of the percentage of voids in the canal filling of a calcium silicate-based sealer and gutta percha cones using two obturation techniques. Materials. 2017;10(10):1170.
https://doi.org/10.3390/ma10101170, PMid:29023402 PMCid:PMC5666976
10. Kim J-A, Hwang Y-C, Rosa V, Yu M-K, Lee K-W, Min K-S. Root canal filling quality of a premixed calcium silicate endodontic sealer applied using gutta-percha cone-mediated ultrasonic activation. Journal of endodontics. 2018;44(1):133-8.
https://doi.org/10.1016/j.joen.2017.07.023, PMid:29102078
11. Yazdi KA, Aminsobhani M, Alemi P. Comparing the ability of different materials and techniques in filling artificial internal resorption cavities. European endodontic journal. 2019;4(1):21-7. https://doi.org/10.14744/eej.2018.13008, PMid:32161882 PMCid:PMC7006561
12. Patel D, Sherriff M, Ford TP, Watson T, Mannocci F. The penetration of RealSeal primer and Tubliseal into root canal dentinal tubules: a confocal microscopic study. International endodontic journal. 2007;40(1):67-71. https://doi.org/10.1111/j.1365-2591.2006.01184.x
13. Sagsen B, Ustün Y, Demirbuga S, Pala K. Push‐out bond strength of two new calcium silicate‐based endodontic sealers to root canal dentine. International endodontic journal. 2011;44(12):1088-91. https://doi.org/10.1111/j.1365-2591.2011.01925.x
14. Turkyilmaz A, Erdemir A. Comparison of dentin penetration ability of different root canal sealers used with different obturation methods. Microscopy Research and Technique. 2020;83(12):1544-51. https://doi.org/10.1002/jemt.23548
15. Jafari F, Samadi Kafil H, Jafari S, Aghazadeh M, Momeni T. Antibacterial Activity of MTA Fillapex and AH 26 Root Canal Sealers at Different Time Intervals. Iran Endod J 2016 [acceso: 14/01/2019]; 11 (3).
16. Mohammadi Z, Giardino L, Palazzi F, Shalavi S. Antibacterial activity of a new mineral trioxide aggregate-based root canal sealer. International dental journal. 2012;62(2):70-3. https://doi.org/10.1111/j.1875-595X.2011.00090.x , PMid:22420474 PMCid:PMC9374948
17. Milani AS, Firuzi S, Barhaghi MHS, Shahi S, Abdollahi AA. Evaluation of sealing abilitiy of mineral trioxide aggregate mixed with propylene glycol as a root canal sealer: A: in vitro: study. Dental research journal. 2019;16(4):216-20.
https://doi.org/10.4103/1735-3327.261124, PMid:31303874 PMCid:PMC6596174
18. Drukteinis S, Peciuliene V, Maneliene R, Bendinskaite R. In vitro study of microbial leakage in roots filled with EndoREZ sealer/EndoREZ Points and AH Plus sealer/conventional gutta-percha points. Stomatologija. 2009;11(1):21-5
19. Adanir N, Cobankara FK, Belli S. Sealing properties of different resin‐based root canal sealers. Journal of Biomedical Materials Research Part B: Applied Biomaterials: An Official Journal of The Society for Biomaterials, The Japanese Society for Biomaterials, and The Australian Society for Biomaterials and the Korean Society for Biomaterials. 2006;77(1):1-4. https://doi.org/10.1002/jbm.b.30408
20. Samiei M, Aghazade M, Farhadi F, Shahveghar N, Torab A, Pakdel SMV. Sealing efficacy of single-cone obturation technique with MTA and CEM cement: an in vitro bacterial leakage study. Journal of dental research, dental clinics, dental prospects. 2014;8(2):77.
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |